Welcome to the 101st edition of the Research Digest. This month’s edition features articles that explore exercise pathophysiology through invasive cardiopulmonary exercise testing, the role of orthostatic hemodynamic changes in cognitive impairment in long COVID and ME/CFS, and clinical guidance for the diagnosis and management of ME/CFS. You can also join our community and choose to have the Digest delivered straight to your inbox at the end of every month, by signing up to our mailing list here. We appreciate the support of everyone who reads the Digest – we encourage regular subscribers to support us with a monthly suggested donation of $2.
Contributing Digesters: Sarah and Shan
Digest Editor: Simone Eyssens
Exercise Pathophysiology in Myalgic Encephalomyelitis/Chronic Fatigue Syndrome and Postacute Sequelae of SARS-CoV-2 - More in Common Than Not?
Authors: Joseph P, Singh I, Oliviera R, Capone CA, Mullen MP, Cook DB, … Systrom DM (Harvard Medical School, Boston, USA)
Publication: Chest Journal
Link: https://doi.org/10.1016/j.chest.2023.03.049
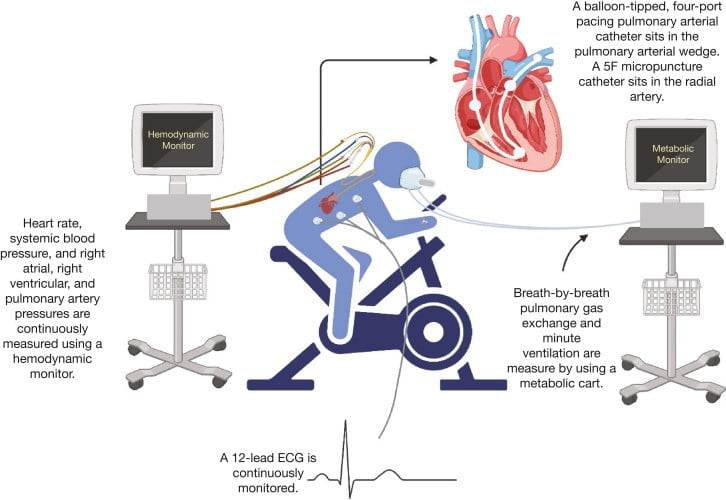
The aim of this review was to examine the capacity of invasive and noninvasive cardiopulmonary tests (iCPETs and niCPETs) to assess ME/CFS and post-acute sequelae of COVID-19 (PASC); the commonalities between both conditions, including small fiber neuropathies (SFN), dyspnea, and mitochondrial dysfunction; how symptoms in children differed to adults; and future directions. niCPET studies found that inefficient breathing in ME/CFS patients led to lower peak oxygen uptake (VO2) than in controls. Serial niCPETS (24 hours apart) assessed recovery and PEM, showing further VO2 reduction, lowered levels of exercise tolerance, and earlier anabolic thresholds (AT) in ME/CFS patients. Behavioural and psychological studies found worsened brain function, pain levels, metabolite and immune activity, and further changes to the gut microbiome. Some papers described chronotropic incompetence in both ME/CFS and PASC, but this was not shown in other larger studies.
The aim of this review was to examine the capacity of invasive and noninvasive cardiopulmonary tests (iCPETs and niCPETs) to assess ME/CFS and post-acute sequelae of COVID-19 (PASC); the commonalities between both conditions, including small fiber neuropathies (SFN), dyspnea, and mitochondrial dysfunction; how symptoms in children differed to adults; and future directions. niCPET studies found that inefficient breathing in ME/CFS patients led to lower peak oxygen uptake (VO2) than in controls. Serial niCPETS (24 hours apart) assessed recovery and PEM, showing further VO2 reduction, lowered levels of exercise tolerance, and earlier anabolic thresholds (AT) in ME/CFS patients. Behavioural and psychological studies found worsened brain function, pain levels, metabolite and immune activity, and further changes to the gut microbiome. Some papers described chronotropic incompetence in both ME/CFS and PASC, but this was not shown in other larger studies.
Whilst deconditioning is often provided as the primary explanation of post-exertional malaise, orthostatic intolerance, and dyspnea in people with ME/CFS and PASC, iCPETs show this to be either incorrect or not the sole reason for these symptoms. Examination of cardiac output (Qc) demonstrates altered aerobic and anaerobic capacity, various cardiac limitations, and circulatory dysregulation. Qc is comparable for ME/CFS and PASC. Biopsies show a prevalence of small fiber neuropathy (SFN) in 33% of ME/CFS patients and up to 90% of PASC patients. The Qc/VO2 ratio distinguishes between preload failure, left-to-right shunt, and mitochondrial dysfunction. Contrary to deconditioning, dyspnea was shown to be entirely due to neurovascular dysregulation, hyperventilation and decreased oxygen extraction, not hypovolemia (VD/VT).
Severe covid-19 in children can present as acute respiratory disease syndrome (ARDS), myocarditis, or multisystem inflammatory syndrome in children (MIS-C). However, those who go on to develop PASC display low peak VO2, but no abnormality of inflammatory markers or pulmatory function. The authors recommend testing children for orthostatic intolerance, as well as blood analysis, echocardiograms, pulmonary function tests, and CPETs.
iCPETs offer unique insights that are not demonstrated through testing at rest or through niCPETs. The authors believe widescale, multidisciplinary meta-analyses involving iCPET and metabolomics are needed.
Cognitive impairment in post-acute sequelae of COVID-19 and short duration myalgic encephalomyelitis patients is mediated by orthostatic hemodynamic changes
Authors: Day H, Yellman B, Hammer S, Rond C, Bell J, Abbaszadeh S, … Vernon SD (Bateman Horne Centre, United States)
Publication: Frontiers in Neuroscience
Link: https://www.frontiersin.org/articles/10.3389/fnins.2023.1203514/full
Many patients with ME/CFS and post-acute sequelae of COVID-19 (PASC) experience cognitive impairment. This can include trouble with concentration, remembering and decision making. This study sought to determine whether orthostatic haemodynamic changes were associated to cognitive impairment in ME/CFS and PASC.
This study utilised a prospective, observational cohort method, and included 256 participants, in three groups: ME/CFS (140 participants, Institute of Medicine criteria), PASC (34 participants) and healthy controls (82 participants). The ME/CFS group was further divided into two subgroups: illness duration less than four years (71 participants) and illness duration greater than 10 years (69 participants). Participants completed clinical evaluation and assessment, including cognitive efficiency measurements (speed and accuracy of responses). Participants completed a cognitive test before, immediately after, and two and seven days after the orthostatic challenge. The orthostatic challenge was a 10-minute NASA lean test, measuring blood pressure and heart rate, and extrapolating pulse pressure and peripheral perfusion.
The authors found that ME/CFS and PASC participants had significantly lower cognitive efficiency scores immediately after the orthostatic challenge, when compared to healthy controls. In ME/CFS participants with disease duration of greater than 10 years, these scores remained low at two and seven days following the orthostatic challenge. Narrow pulse pressure was observed in PASC and ME/CFS participants, and in PASC participants this was associated with slowed information processing compared to healthy controls. Increased heart rate and decreased procedural reaction was observed during the orthostatic challenge in PASC and some ME/CFS participants with disease duration of less than four years.
PASC participants were seen to experience haemodynamic changes during orthostatic challenge that were associated with slowed reaction time and reduced response accuracy. ME/CFS participants with disease duration of less than 4 years experienced reduced cognitive efficiency associated with elevated heart rate in response to orthostatic challenge. ME/CFS participants with disease duration of greater than 10 years experienced cognitive impairment, but this was not correlated with haemodynamic changes associated with orthostatic challenge. The authors suggest that these findings highlight the necessity of early diagnosis to reduce the impact of haemodynamic and other physiological effects on cognitive impairment symptoms.
Diagnosis and management of myalgic encephalomyelitis/chronic fatigue syndrome
Authors: Grach SL, Seltzer J, Chon TY, & Ganesh R (Mayo Clinic, United States)
Publication: Mayo Clinic Proceedings
Link: https://www.mayoclinicproceedings.org/article/S0025-6196(23)00402-0/fulltext
There has been an increased interest in ME/CFS as up to 50% of patients with post-COVID syndrome go on to fulfil the criteria for ME/CFS. This review sought to describe a generalist approach to the diagnosis and management of ME/CFS.
Epidemiology/Etiology
- ME/CFS affects all ages, genders, races and socioeconomic backgrounds. Presentation may differ in men compared to women, potentially resulting in underdiagnosis in men.
- Up to 80% of ME/CFS cases are preceded by an infection, most commonly viral, or by multiple smaller events followed by a final trigger causing clear onset.
Diagnosis
- ME/CFS is a diagnosis based on the presence of particular signs and symptoms, not a diagnosis of exclusion. The US Centres for Disease Control and Prevention recommend the 2015 Institute of Medicine ME/CFS diagnostic criteria.
- The lack of diagnostic biomarkers, similarity to other diseases, and reduced clinician awareness of ME/CFS contribute to delayed diagnosis – approximately one third of ME/CFS patients waited at least 5 years for their diagnosis.
- Although ME/CFS is present across a spectrum of mild (approximately 25% of ME/CFS patients), moderate (50%) to severe and very severe (25%), the IOM criteria require a 50% decrease in pre-illness capacity in order to be diagnosed.
Practical considerations in diagnosis
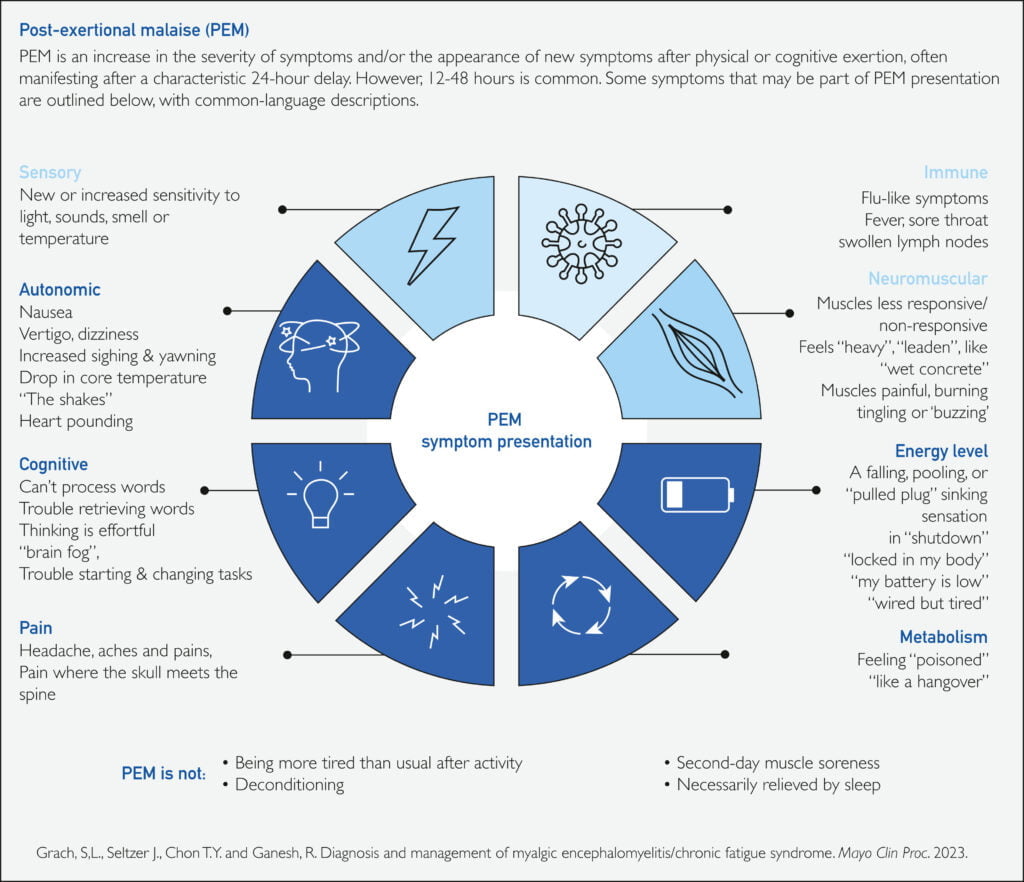
- Patient history: patients often report a wide range of symptoms, it is necessary to determine whether symptoms fulfil the ME/CFS diagnostic criteria. Post-exertional malaise (PEM) is a defining characteristic of ME/CFS.
- Risk factors for ME/CFS: female sex, age 10-19 or 30-39, infection (especially viral), preexisting or family history of autoimmune disease, neurologic or other multisystem chronic disease.
Co-morbidities
- 75-80% of ME/CFS patients report at least one other disease. The most commonly seen co-morbid diseases/disorders include hypermobile Ehlers-Danlos Syndrome, postural orthostatic tachycardia syndrome and other autonomic disorders, and mast cell activation syndrome.
General management
- Managing energy expenditure and avoiding PEM through effective pacing may lead to improvements in functional ability over time and improved quality of life. Identifying the heart rate threshold that triggers PEM and staying below this level may assist self-management.
- Pacing does not involve systematic increases in activity, and is not curative.
- Graded exercise therapy has not been proven to be effective for ME/CFS.
- Pharmacological medications or supplements may assist with symptom management. Patients are often sensitive to medications and may need to be started on a low dose, with gradual increase in dose over time.
Calls for more inclusive disaster planning
Authors: Gwynn L
Publication: ABC News
Link: https://www.abc.net.au/news/2023-11-19/calls-for-more-inclusive-disaster-planning/103114376
Community organisation Australia reMade has released a report urging a new approach to emergency preparedness, one that ensures that everyone is included, including people with disabilities.
Kate Herbert, a nurse who lives with ME/CFS, says it’s important that people with chronic illness, are neurodivergent or have a disability have their needs met before, during and after an emergency.
Australia reMade co-Director Dr Millie Rooney said, “We found there is a need for people to be seen, safe and supported during and after a crisis, and that their communities already need to be strong and connected before disaster strikes for this to occur. Inequality exacerbates the impact of disaster, so if we address that before disaster then we have less work to do in recovery.”


