Summary
Although exercise therapy has historically been recommended as a primary treatment for ME/CFS, and is increasingly promoted for long COVID, the supporting evidence is limited, particularly in cases where post-exertional malaise (PEM) is present. Studies indicate that exercise therapy may not be effective for people with ME/CFS or long COVID who experience PEM. Additionally, patient surveys have consistently found that the majority of individuals with ME/CFS report harm from graded exercise therapy (GET), which can include short or long-term decline in function.
Emerge Australia advocates a “do no harm” approach to managing ME/CFS and long COVID. Until effective treatments are identified, pacing and symptom management remain the safest and most appropriate strategies.
Some people with PEM may be able to do limited physical activity, but this must be approached with caution. Any exercise should be undertaken within the person’s energy limits and should not be seen as a treatment for the underlying condition.
Background / What is the issue?
Graded exercise therapy (GET) has historically been the primary treatment recommended for ME/CFS, both in Australia and internationally [1,2]. This recommendation was based on the belief that ME/CFS symptoms were primarily cause by physical deconditioning [3] or sensitisation of the central nervous system [4].
These models ignored the evidence of biological abnormalities found in ME/CFS [5,6] and assumed that symptoms were driven by behaviour. According to these models, people with ME/CFS were in a vicious cycle: they avoided activity to minimise symptoms, which led to further deconditioning or sensitisation, worsening symptoms and continued avoidance. GET was developed to break this cycle by gradually increasing physical fitness or reducing nervous system sensitivity through structured, incremental exposure to exercise [4,7].
Although GET has been widely recommended for many years, it has been controversial because many people with ME/CFS consistently report a worsening of symptoms after this treatment [8,9]. Patient reports of harm are supported by biomedical research, which shows abnormal physiological responses to exercise [10].
Despite these concerns, people with ME/CFS in Australia are often required to undertake GET to access much-needed supports like Disability Support Pension (DSP) and National Disability Insurance Scheme (NDIS).
In recent years, GET has also been recommended as a treatment for long COVID, though it is similarly controversial.
What does the evidence say?
At first glance, the evidence appears to support GET for ME/CFS. The current Cochrane review for “Exercise therapy for chronic fatigue syndrome” states that “Exercise therapy probably has a positive effect on fatigue in adults with CFS compared to usual care or passive therapies” [11].
However, there are significant flaws in GET research that must be considered when interpreting these results [12,13]. Key issues include:
- Broad diagnostic criteria: Many studies use broad definitions of ME/CFS, which may include few or no participants who experience post-exertional malaise (PEM) – a core symptom of the condition.
- Subjective outcomes in unblinded trials: Most studies rely on self-reported outcomes without blinding, which introduces a high risk of bias and would not be acceptable in drug trials. When objective outcome measures are included in GET trials, they typically show little or no improvement.
- Inadequate reporting of harm: Clinical trials of GET often fail to adequately report adverse effects. This contributes to the false perception that GET is safe for all people with ME/CFS or long COVID. However, patient surveys from around the world consistently show that a majority of people with ME/CFS report feeling worse after GET, with some experiencing permanent harm.
When these flaws are taken into account, detailed analyses of clinical trials show that GET is not effective, does not support the deconditioning or central sensitisation hypotheses, and carries a risk of harm to people living with ME/CFS or long COVID [12,13].
Note: In 2018, the current Cochrane review was the subject of a formal complaint regarding its scientific methods and conclusions. The complaint was upheld, and in 2019 the review amended to address some of the concerns. That same year, Cochrane’s then Editor-in-Chief acknowledged that the amended review relied on outdated methods and definitions and announced that a new review would be developed [14]. However, in late 2024, Cochrane announced it would no longer proceed with a new review and has not withdrawn the existing one, despite its acknowledged flaws [15].
1. Broad diagnostic criteria
Post-exertional malaise (PEM) is the hallmark symptom of ME/CFS and is also common in long COVID. PEM refers to the worsening of symptoms after even minor physical or mental effort. It involves more than just fatigue — symptoms such as pain, cognitive dysfunction, and sensory sensitivities can worsen, often with a delayed onset and prolonged recovery.
PEM can be objectively measured using two-day cardiopulmonary exercise testing (CPET). Studies have shown that people who experience PEM are unable to reproduce their performance on the second day of maximal effort testing, due to the physiological effects of exertion on the first day [16]. This pattern is not seen in healthy controls or people with multiple sclerosis, and cannot be explained by lack of effort [16,17].
Although PEM is central to the diagnosis of ME/CFS, most GET studies use broad diagnostic criteria that do not require PEM as a mandatory symptom [12,18]. As a result, it is unclear how many participants in these studies actually experienced PEM. Despite this, the findings of these studies are often generalised to all people with ME/CFS and long COVID, including those who do experience PEM.
This raises serious concerns about the validity of applying GET to individuals who experience PEM. Broad inclusion criteria increase the risk of enrolling participants with other conditions that may respond positively to exercise, such as depression [12].
2. Subjective outcomes in unblinded trials
GET studies are unblinded, as participants know whether they are receiving the intervention. When trials are unblinded and rely on subjective outcome measures (such as self-reported fatigue or function), the results carry a high risk of response bias. Participants may unconsciously adjust their responses to align with perceived expectations, either their own or the researchers’, which can skew outcomes [19,20].
Research shows that unblinded trials with subjective outcomes tend to overestimate treatment effects[19,21]. In contrast, unblinded trials that use objective outcome measures do not show the same level of bias [22]. One review concluded:
“Clinical and policy decisions should not be based on trials in which blinding is not feasible and outcome measures are subjectively assessed. Where blinding is not possible, trials should use objective outcomes and blind outcome assessors wherever possible” [21].
Despite being unblinded, most GET trials rely on subjective rating scales as their primary outcomes. While these trials often report modest improvements on subjective outcomes, objective outcome measures show little or no improvement [22].
Of the eight trials in the current Cochrane review, seven included objective outcome measures. Only two of these trials showed any improvement on these measures, and the gains were minimal (4-7% improvement) [12].
The PACE trial, the largest GET trial ever conducted, included a six-minute walk test and a step test. The step test showed no significant improvement [23]. The six-minute walk test showed an average improvement of 67 metres, with participants walking an average of 379 metres post-treatment. This distance is comparable to that of individuals with heart failure, and far below the 500–700 metres typical of healthy adults [12,24].
Given the lack of blinding and limitations of subjective outcome measures in such trials, the results of the objective outcome measures should be viewed as the most reliable indicator of treatment effect. These showed minimal or no improvement.
The poor results on objective measures challenge both the deconditioning and central sensitisation models of ME/CFS. If GET were effective, it would be expected to significantly improve physical fitness and reduce post-exertional malaise (PEM). The evidence does not support this. Furthermore, long-term follow-up shows that any short-term gains on subjective measures do not last. At follow-up, there is often no significant difference between those who received GET and those who did not [22].
3. Inadequate reporting masks risk of harm
Although proponents of GET often claim the treatment is safe for people with ME/CFS, this is not supported by evidence. Numerous reviews have criticised GET studies for inadequate harm reporting [25]. GET study designs may also discourage accurate reporting of adverse effects, as participants are frequently told to interpret symptom exacerbation as a normal part of recovery [7,22]. This may contribute to underreporting of harms and obscure the true risks of the intervention.
In contrast, independent surveys of people living with ME/CFS consistently report high levels of harm following GET:
Australia: Emerge Australia’s Health and Wellbeing Survey (2015) found that 89% of 586 respondents reported feeling worse after exercise or increased activity [8].
UK: 74% of 1,428 survey respondents reported feeling worse after GET [9].
Norway: Two-thirds of 1,096 survey respondents reported feeling worse after GET, with half saying they felt seriously worse [26].
Netherlands: In a 2023 survey of over 1,500 people with ME/CFS, GET was ranked as the least helpful treatment, with many respondents reporting feeling worse after the treatment [27].
4. Illness severity
Most exercise trials do not account for differences in illness severity [28]. What may be safe for someone with mild ME/CFS could be harmful or even dangerous for those with moderate or severe illness. Despite this, GET is often recommended broadly to anyone with ME/CFS or long COVID, without considering individual capacity or severity. This highlights the need for extreme caution when interpreting the findings of any exercise-based intervention in this population.
5. First do no harm
While patient surveys are not as highly regarded as clinical trials, their findings deserve consideration due to the consistency of results and the supporting biomedical evidence for PEM. In medicine, the principle is first do no harm. The weak evidence supporting GET, combined with consistent reports of harm, should give health professionals serious pause before recommending this treatment for people with ME/CFS or Long COVID who experience PEM. The risks are high and potential benefits uncertain.
Concerns about GET’s effectiveness, along with ongoing patient reports of harm, have led the US Centers for Disease Control and Prevention (CDC) and the UK National Institute for Health and Care (NICE) to withdraw their support for these treatments for ME/CFS, and caution against exercise programs with fixed increments [31,32]. However, clinical guidance in Australia continues to recommend GET, putting Australia out of step with international best practice.
The Royal Australian College of General Practitioners’ First Do No Harm traffic light system advises GPs to avoid Red Traffic Light actions — interventions which lack benefit and may cause harm [33]. The high rates of reported harm and lack of strong supporting evidence mean GET fits the definition of a Red Traffic Light action. Emerge Australia believes it should not be prescribed to this population in any form.
Given the weak evidence and significant risk of harm, Australians with ME/CFS or long COVID who experience PEM should not be required to undergo GET to access supports like the NDIS or DSP. Forcing them to do so breaches human rights by denying the individual’s right to refuse medical treatment, especially one likely to cause harm.
Is exercise ever safe or appropriate for people with ME/CFS or long COVID who experience PEM?
Exercise is not an effective treatment or cure for ME/CFS. However, some people with ME/CFS may choose to include gentle movement or exercise to help maintain or improve functional strength, and range of motion and physical capacity [28].
Managing within energy limits
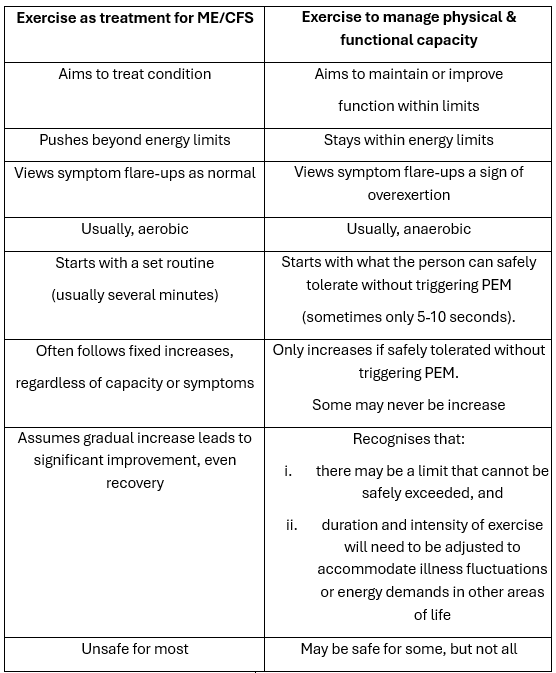
This approach differs from GET and traditional forms of rehabilitation, as it does not aim to treat the underlying condition or push beyond limits. Instead, it focuses on working within the person’s available energy reserves. This must be approached with great care.
For those who choose to try to exercise in this way, safety is essential. Exercise is best undertaken under the supervision of a suitably qualified health professional who understands PEM and the potential risks. While some may be able to manage short periods of gentle activity, for others, even minimal exertion may exceed their energy limits and cause harm.
Emerge Australia’s Position
Evidence shows that graded exercise therapy (GET) is not an effective treatment for ME/CFS or long COVID, when post-exertional malaise (PEM) is present. Given the consistent reports of harm from patients, GET also carries a significant risk.
While individualised exercise programs may help maintain or improve functional capacity for some people with ME/CFS or long COVID, they should not be considered treatments that can remedy or ‘cure’ the underlying condition. Because any activity, including exercise, can cause PEM, tailored exercise must be approached with caution, implemented within the patient’s energy capacity, be carefully monitored and regularly reviewed. The risks and benefits should always be clearly explained so that patients can give informed consent. People with more severe ME/CFS or long COVID may not be able to engage with any form of exercise.
Given that graded exercise therapy (GET) has been shown to be ineffective and potentially harmful, Australians with ME/CFS and long COVID should not be required to undergo GET in order to access necessary supports like the Disability Support Pension (DSP) or National Disability Insurance Scheme (NDIS). Forcing them to do so breaches human rights by denying the individual’s right to refuse medical treatment.
1. Working group of The Royal Australasian College of Physicians (RACP). Clinical practice guideline: Chronic Fatigue Syndrome. . Med J Aust 177, 51–52 (2022).
2. National Institute for Health & Care Excellence. Chronic fatigue syndrome/myalgic encephalomyelitis (or encephalopathy): Diagnosis and management. (2007).
3. White, P. D. et al. Comparison of adaptive pacing therapy, cognitive behaviour therapy, graded exercise therapy, and specialist medical care for chronic fatigue syndrome (PACE): A randomised trial. The Lancet 377, (2011).
4. Lloyd, A. R. & Meer, J. W. M. v. d. The long wait for a breakthrough in chronic fatigue syndrome. BMJ 350, h2087–h2087 (2015).
5. Komaroff, A. L. & Lipkin, W. I. Insights from myalgic encephalomyelitis/chronic fatigue syndrome may help unravel the pathogenesis of postacute COVID-19 syndrome. Trends Mol Med 27, 895–906 (2021).
6. Komaroff, A. L. & Lipkin, W. I. ME/CFS and Long COVID share similar symptoms and biological abnormalities: road map to the literature. Front Med (Lausanne) 10, 1187163 (2023).
7. Bavinton, J. , D. L. , & W. P. Manual for Therapists: Graded Exercise Therapy for CFS/ME. (https://www.qmul.ac.uk/wiph/media/the-wolfson-institute-of-population-health-wiph/documents/5.get-therapist-manual.pdf, 2004).
8. Emerge Australia. Health and Wellbeing Study . https://emerge.org.au/health-and-wellbeing-survey-2015/ 1–77 (2015).
9. Geraghty, K., Hann, M. & Kurtev, S. Myalgic encephalomyelitis/chronic fatigue syndrome patients’ reports of symptom changes following cognitive behavioural therapy, graded exercise therapy and pacing treatments: Analysis of a primary survey compared with secondary surveys. J Health Psychol 24, (2019).
10. Moore, G. E. et al. Recovery from Exercise in Persons with Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (ME/CFS). Medicina (B Aires) 59, (2023).
11. Larun, L., Brurberg, K. G., Odgaard-Jensen, J. & Price, J. R. Exercise therapy for chronic fatigue syndrome. Cochrane Database of Systematic Reviews 2021, (2019).
12. Vink, M. & Vink-Niese, A. Graded exercise therapy for myalgic encephalomyelitis/chronic fatigue syndrome is not effective and unsafe. Re-analysis of a Cochrane review. Health Psychol Open 5, 205510291880518 (2018).
13. Vink, M. & Vink-Niese, A. The Updated NICE Guidance Exposed the Serious Flaws in CBT and Graded Exercise Therapy Trials for ME/CFS. Healthcare (Basel) 10, (2022).
14. Cochrane. Publication of the Cochrane Review: Exercise therapy for chronic fatigue syndrome. https://www.cochrane.org/about-us/news/cfs (2019).
15. Cochrane. Update on ‘Exercise therapy for chronic fatigue syndrome’. . https://www.cochrane.org/about-us/news/update-exercise-therapy-chronic-fatigue-syndrome (2024).
16. Keller, B. A., Pryor, J. L. & Giloteaux, L. Inability of myalgic encephalomyelitis/chronic fatigue syndrome patients to reproduce VO2peak indicates functional impairment. J Transl Med 12, (2014).
17. Hodges, L. Repeated Cardiopulmonary Exercise Testing of ME/CFS Patients. in 163–172 (2025). doi:10.1007/978-1-0716-4498-0_10.
18. Vink, M. & Vink-Niese, F. Graded exercise therapy does not restore the ability to work in ME/CFS – Rethinking of a Cochrane review. Work 66, 283–308 (2020).
19. Hróbjartsson, A. et al. Observer bias in randomised clinical trials with binary outcomes: systematic review of trials with both blinded and non-blinded outcome assessors. BMJ 344, e1119 (2012).
20. Wechsler, M. E. et al. Active Albuterol or Placebo, Sham Acupuncture, or No Intervention in Asthma. New England Journal of Medicine 365, 119–126 (2011).
21. Savović, J. et al. Influence of reported study design characteristics on intervention effect estimates from randomized, controlled trials. Ann Intern Med 157, 429–38 (2012).
22. Tack, M., Tuller, D. M. & Struthers, C. Bias caused by reliance on patient-reported outcome measures in non-blinded randomized trials: an in-depth look at exercise therapy for chronic fatigue syndrome. Fatigue 8, 181–192 (2020).
23. Wilshire, C. E. et al. Rethinking the treatment of chronic fatigue syndrome-a reanalysis and evaluation of findings from a recent major trial of graded exercise and CBT. BMC Psychol 6, 6 (2018).
24. Rasekaba, T., Lee, A. L., Naughton, M. T., Williams, T. J. & Holland, A. E. The six‐minute walk test: a useful metric for the cardiopulmonary patient. Intern Med J 39, 495–501 (2009).
25. Agency for Healthcare Research and Quality U.S. Department of Health and Human Services. Diagnosis and Treatment of Myalgic Encephalomyelitis/Chronic Fatigue Syndrome. (2016).
26. Bringsli, G. J. , G. A. & W. B. K. G. The Norwegian ME Association National Survey Abridged English Version. https://www.me-foreningen.no/wp-content/uploads/2016/09/ME-Nat-Norwegian-Survey-Abr-Eng-Ver.pdf 1–9 (2014).
27. Patiëntenfederatie Nederland. Ervaringen met ME/CVS. . https://www.steungroep.nl/images/ME_CVS_en_wetenschap/Definitieve%20rapportage%20ervaringen%20met%20MECVS%20-%20maart%202024.pdf 1–90 (2024).
28. Clague-Baker, Nicola., Hilliard, Natalie., Bull, Michelle. & Leslie, Karen. A Physiotherapist’s Guide to Understanding and Managing ME/CFS. (Jessica Kingsley Publishers, 2023).
29. Tuller, D. & Vink, M. Graded exercise therapy and cognitive behavior therapy do not improve employment outcomes in ME/CFS. Work 74, 1235–1239 (2023).
30. McPhee, G., Baldwin, A., Kindlon, T. & Hughes, B. M. Monitoring treatment harm in myalgic encephalomyelitis/chronic fatigue syndrome: A freedom-of-information study of National Health Service specialist centres in England. J Health Psychol 26, 975–984 (2021).
31. Centers for Disease Control & Prevention. Manage Myalgic Encephalomyelitis/Chronic Fatigue Syndrome – Overview: treatment and management. https://www.cdc.gov/me-cfs/management/index.html (2024).
32. National Institute for Health and Care Excellence. Myalgic encephalomyelitis (or encephalopathy)/chronic fatigue syndrome: diagnosis and management. . https://www.nice.org.uk/guidance/ng206 (2021).
33. Royal Australian College of General Practitioners (nd). Traffic light system. https://www.racgp.org.au/clinical-resources/clinical-guidelines/key-racgp-guidelines/view-all-racgp-guidelines/first-do-no-harm/about-first-do-no-harm/traffic-light-system (2022).
